
More Information
Submitted: February 02, 2026 | Accepted: February 11, 2026 | Published: February 13, 2026
Citation: Kravchenko IV, Vinnikova IN, Sevryukov VT, Boyarintseva VA. Optimization of Therapy in Patients with Paranoid Schizophrenia and Non-suicidal Autoaggression who have recovered from Coronavirus Infection. Arch Psychiatr Ment Health. 2026; 10(1): 001-005. Available from:
https://dx.doi.org/10.29328/journal.apmh.1001060
DOI: 10.29328/journal.apmh.1001060
Copyright license: © 2026 Kravchenko IV, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Comorbidity; Coronavirus infection; Osmotic dehydration therapy; Paranoid schizophrenia; Non-suicidal autoaggressive behavior

Optimization of Therapy in Patients with Paranoid Schizophrenia and Non-suicidal Autoaggression who have recovered from Coronavirus Infection
Kravchenko IV1* , Vinnikova IN2, Sevryukov VT3 and Boyarintseva VA4
, Vinnikova IN2, Sevryukov VT3 and Boyarintseva VA4
1Interdistrict Center for Medical Rehabilitation at the State Budgetary Healthcare Institution “Polyclinic No. 38”, St. Petersburg, Russia
2Federal State Budgetary Institution “National Medical Research Center for Psychiatry and Narcology named after V. P. Serbsky” of the Ministry of Health of the Russian Federation
3Department of Forensic Medicine, North-Western State Medical University Named After I.I. Mechnikova, Russia
4St. Petersburg City Center for Early Childhood Intervention for Autism Spectrum Disorders, St. Petersburg, Russia
*Corresponding author: Igor Vladimirovich Kravchenko, MD, PhD, Psychiatrist, Forensic Psychiatric Expert, Psychotherapist, Clinical Pharmacologist of the Interdistrict Center for Medical Rehabilitation at the State Budgetary Healthcare Institution “Polyclinic No. 38”, St. Petersburg, Russia, Email: [email protected]
The issue of comorbidity of coronavirus infection and chronic mental disorders remains an important medical problem, determining the relevance of the study. A continuous, non-randomized method was used to conduct a comparative analysis of combination therapy in 124 patients with paranoid schizophrenia with non-suicidal autoaggressive behavior (abbreviated NAAB) who have had coronavirus infection. A clinical method and experimental psychometric research methods were used, including brief psychiatric assessment scales; social functioning scales and a visual analog pain scale. The clinical picture features during the period of remote consequences of the transferred coronavirus infection in the examined persons were established. It was established that antipsychotics in combination with non-steroidal anti-inflammatory drugs have a positive clinical effect in the examined persons.
Moreover, additional administration of drugs with osmotic dehydrating activity statistically significantly increases the clinical effect of the treatment in relation to the leading psychopathological features, including NSAB in this group of patients.
The consequences of coronavirus infection remain a pressing clinical problem due to its ability to change the course of many chronic mental disorders, including paranoid schizophrenia [1-3]. The dominant theory of the pathogenesis of post-COVID changes is the ability of infection to cause inflammatory and autoimmune changes that are difficult to reverse and tend to last for a long time, accompanied by hypoxia and apoptosis of nerve cells [4-7]. Such changes lead to the formation of residual organic changes in the brain in the form of stable general cerebral and focal neurological disorders. In addition, such patients experience an increase in cognitive and behavioral disorders, including non-suicidal autoaggressive behavior, or “NSAB” for short [8-11]. One of the methods of correction of comorbid post-infectious changes is symptomatic use of drugs of the group of non-steroidal anti-inflammatory drugs (abbreviated NSAIDs). However, such drugs have low clinical effectiveness, are prescribed in short courses due to the ability to cause a wide range of side effects. Another way to solve this clinical problem may be the administration of osmotic dehydrating drugs. Medicines of this class have proven themselves to be positive during many years of use in the treatment of post-infectious complications of various etiologies [12-14]. To confirm or refute the hypothesis about the clinical feasibility of using osmotic dehydrating drugs in the complex therapy of patients with paranoid schizophrenia with NSAB who have had coronavirus infection, this study was conducted. The aim of the study: to clarify the role of osmotic dehydrating drugs in the complex therapy of patients with paranoid schizophrenia with NSAB who have had coronavirus infection.
A non-randomized method was used to conduct a comparative analysis of combination therapy in 124 patients with paranoid schizophrenia with NSAB who had coronavirus infection. All subjects were men aged 20 to 60 years. The average age of the subjects was 34.1 ± 1.1 years. The average duration of the procedural disease was 18.2 ± 1.5 years. Type of schizophrenic process: continuous – progressive. Inclusion criteria were: 1) compliance of the diagnosis of paranoid schizophrenia with the criteria of ICD-10 revision (F20.0); 2) state of clinical remission; 3) clinical signs of NSAВ in the examined individuals; 4) immunologically confirmed coronavirus infection suffered no earlier than 12 months prior to inclusion in the study; 5) the course of coronavirus infection corresponded to moderate or severe severity; The severity of the coronavirus infection was determined by clinical guidelines for the diagnosis of coronavirus infection in force in the Russian Federation. Moderate severity of COVID infection corresponded to at least two of the following four main criteria: 1. Body temperature ≥ 38.0 °C 2. Blood oxygenation < 95% 3. Heart rate > 22/min 4. Serum C-reactive protein > 10 mg/L CT scan data: changes in lung tissue, from 25 to 50%. Severe COVID infection severity met at least two of the following four main criteria: body temperature ≥39 ºС 2. Respiratory rate ≥30 per minute 3. Blood oxygenation ≤ 93%4. Additional criteria: confusion, agitation; unstable hemodynamics (systolic blood pressure < 90 mm Hg, or diastolic blood pressure < 60 mm Hg; diuresis < 20 ml per hour); computed tomography data: changes in lung tissue - from 50 to 75% and higher. Arterial blood lactate > 2 mmol / l [15]. The exclusion criteria were: 1) psychotic level of disorders at the time of inclusion in the study; 2) mild course of coronavirus infection; 3) use of any drug before inclusion in the study. The choice of drugs was determined by their most frequent use in practice work in this group of patients. Quetiapine was used as an antipsychotic. Non-specific symptomatic therapy was limited to the administration of diclofenac; Acetazolamide and mannitol were used as osmotic dehydrating agents. Quetiapine, diclofenac, and acetazolamide were administered orally. Mannitol was administered intravenously. The mental state of the examination was assessed clinically at the time of inclusion in the study (day 1), then on days 21 and 42 of the study. Clinical assessment of the condition of the subjects, including a comparative analysis of the frequency of NSAB, was performed 42 days before and after inclusion in the study. To objectify the obtained data, the Brief Psychiatric Assessment Scale, the Social Functioning Scale, and the visual analogue scale (abbreviated: VAS scale) were used. Because the study included small sample sizes, Fisher’s exact test was used to assess statistical error. Fisher criterion. All subjects were randomly divided into 3 comparison groups. Dehydrating drugs were prescribed from the first day of the study, in a course of 7 days with a repeat course of the same duration and doses on the 21st day from the date of the study. The studied drugs were used in the doses presented in Table 1.
| Table 1: Distribution of average daily doses of drugs among subjects. | |
| International nonproprietary names of the drugs used/ number of patients in comparison groups | Average daily doses of drugs (milligram, abbreviated mg) |
| Comparison group 1: quetiapine + diclofenac (42 patients) | 655,6 ± 4,2 mg +150 mg |
| Comparison group 2: quetiapine + diclofenac + acetazolamide (40 patients) | 651,7 ± 2,5 mg +150 мг+ 750 mg |
| Comparison group 3: quetiapine + diclofenac + acetazolamide + mannitol (42 patients) | 681,7 ± 2,1 mg +150 mg ”+ 7 50 mg + 400 mg |
The clinical characteristics of the subjects were as follows. In the pre-COVID period, the clinical picture of the patients examined was determined by an increase in negative procedural changes, with periodic exacerbation of psychotic symptoms. The latter contained elements of protopathic anxiety, psychomotor agitation, and insomnia. Then hallucinatory-delusional disorders in the form of persecution, a feeling of “possession” of thoughts, their “manufacturing and openness to others” intensified. Hallucinatory experiences were predominantly auditory and had an imperative nature. These clinical phenomena corresponded to the criteria of Kandinsky-Clerambault syndrome. During the interictal period, neurocognitive processual changes in the form of atactic thinking, mentism, and sperrung increased. The ability for any purposeful activity was lost, dysfunction of the emotional sphere increased, interpreted as a phenomenon of apathetic-abulic syndrome. NAAB was distinguished by a specific situational focus, the presence of a preparatory period with subsequent application of superficial self-cuts in the area of the forearms, hands. Less often swallowing of small foreign bodies wrapped in a piece of bread was observed. After an act of non-suicidal aggression, a decrease in the severity of psychomotor agitation, the level of conflict, and manifestations of verbal and physical aggression was observed. Criticism of one’s actions was absent. In the post-infectous period, the clinical pathomorphosis consisted of the formation of previously uncharacteristic psychopathological changes. A decrease in the frequency of typical psychotic attacks was noted, which were replaced by clinical manifestations conditionally formed into four syndrome complexes: chronic pain syndrome in the form of cephalgia; Depersonalization-derealization syndrome, as well as catatonic and dysphoric syndromes. Such changes were combined in 98% of patients. Chronic pain syndrome was represented by persistent headaches, described as pressing, aching, localized in the frontal-temporal region. There was a feeling of pressure on the eyes, nausea, and, less frequently, single vomiting that did not bring relief. The pain became more frequent with changes in weather conditions, at elevated ambient temperatures, its average intensity was 7.7 points on the VAS scale, the pain was not relieved by taking NSAIDs. The accompanying background was dizziness, deterioration of concentration and short-term memory, sleep talking, bruxism. The above clinical signs were noted in 119 patients. These symptoms are traditionally in the Russian Neurological School are regarded as manifestations of intracranial hypertension, subject to conservative treatment with osmotic diuretics [16]. The derealization-depersonalization syndrome included phenomena of previously seen, heard, experienced, and told (“deja vu, deja entendu, deja vecu, deja eprouve, deja raconte”). These clinical signs were present in 32 patients. Of these, in 17 patients, similar psychopathological experiences transformed into stable symptom complexes with an increase in protopathic anxiety, psychomotor agitation, manifestations of Kappagra and Fregoli syndromes (psychotic level of disorders). The catatonic syndrome was represented by catatonic stupor (substupor). There was an unmotivated refusal to speak, less often – echolalia (unmotivated repetition of other people’s phrases), as well as the “air cushion symptom” and the phenomenon of “wax flexibility”. Catatonic excitement was not observed. Similar clinical manifestations were diagnosed in 21 patients. The clinical manifestations of dysphoric syndrome were episodes of psychomotor agitation against the background of depressed mood, with elements of irritability, anger and anxiety (121 patients). Psychomotor agitation itself was characterized by impulsiveness, irritability, often without a clear direction, then turning into asthenic weakness and sleep. Non-suicidal self-harm, realized in the structure of dysphoric syndrome, was distinguished by impulsiveness, mainly a single execution with the outcome in motor inhibition, partial forgetting of the period of excitation, formal criticism of what was done.
It was established that all the used treatment regimens had a positive effect on the leading clinical manifestations, differing in the degree of intensity and time of implementation of the clinical response. Clinical changes in chronic pain syndrome were manifested in a decrease in the frequency and intensity of headache attacks, dizziness, and increased weather resistance. The intensity of headache was determined within 3.5 points on the VAS scale. Patients also noted an improvement in short-term memory and concentration. Depersonalization-derealization syndrome was losing a tendency to transition into a psychotic episode. At the clinical level, the manifestations of the syndrome were represented by a short-term and spontaneously passing feeling of unreality of what was happening, a slowdown in the perception of time and movement (“as if time were flowing slowly, a feeling that you were watching yourself from the outside, like in a slow-motion movie”). At the same time, there was a critical assessment of the experiences that were taking place. The catatonic syndrome lost its motor inhibition, phrased speech appeared, and answers were given in terms of the question asked; Echolalia, the “air cushion symptom,” and the “waxy flexibility” phenomenon were reduced. Dysphoric syndrome retained elements of a melancholy-depressed-irritable mood. At the same time, the frequency and intensity of psychomotor agitation, impulsivity, and severity of post-attack asthenia decreased. In the implementation of the NSAB, impulsivity decreased, and conversely, thoughtfulness and planning for the implementation of non-suicidal self-harm returned. It was established that on the 21st day of the study, a decrease in the overall score at the level of trends on the scale of a brief psychiatric assessment was noted in all comparison groups. On the 42nd day of the study, the decrease in the total score on this scale in the first comparison group remained at the level of trends, becoming statistically significant in those examined in the second and third groups (Table 2).
| Table 2: Dynamics of psychopathological changes according to the Mini-Psychiatric Assessment Scale (in points). | |||
| Comparison groups | Stages of therapy | ||
| 1 day | 21 day | 42 day | |
| 1st group | 78,2 | 67,0 F 1.17, p > 0,05 |
57,2 F 1.37, p > 0,05 |
| 2nd group | 78,3 | 61,8 F 1.27, p > 0,05 |
47,5 F 1.65, p < 0,05 |
| 3rd group | 78.4 | 55,2 F 1.42, p > 0,05 |
43,7 F 1.79, p < 0,01 |
It was established that on the 21st day of the study, a decrease in the overall score at the level of trends on the social functioning scale was noted in the first and second comparison groups, becoming statistically significant in those examined in the third group. On the 42nd day of the study, a decrease in the total score on this scale was noted at the level of trends in the first and second comparison groups, becoming statistically significant in those examined in the third group (Table 3).
| Table 3: Dynamics of psychopathological changes on the social functioning scale (in points). | |||
| Comparison groups | Stages of therapy | ||
| 1 day | 21 day | 42 day | |
| 1st group | 38,4 | 44,1 F 1.15, p > 0,05 |
50,2 F 1.31, p > 0,05 |
| 2nd group | 37,9 | 46,6 F 1.23, p > 0,05 |
56.,6 F 1.49, p > 0,05 |
| 3rd group | 34,6 | 53.7 F 1.55, p < 0,05 |
61,5 F 1.78, p < 0,01 |
Finally, positive dynamics were noted in the form of a decrease in the frequency of attacks of non-suicidal autoaggression (Figure 1).
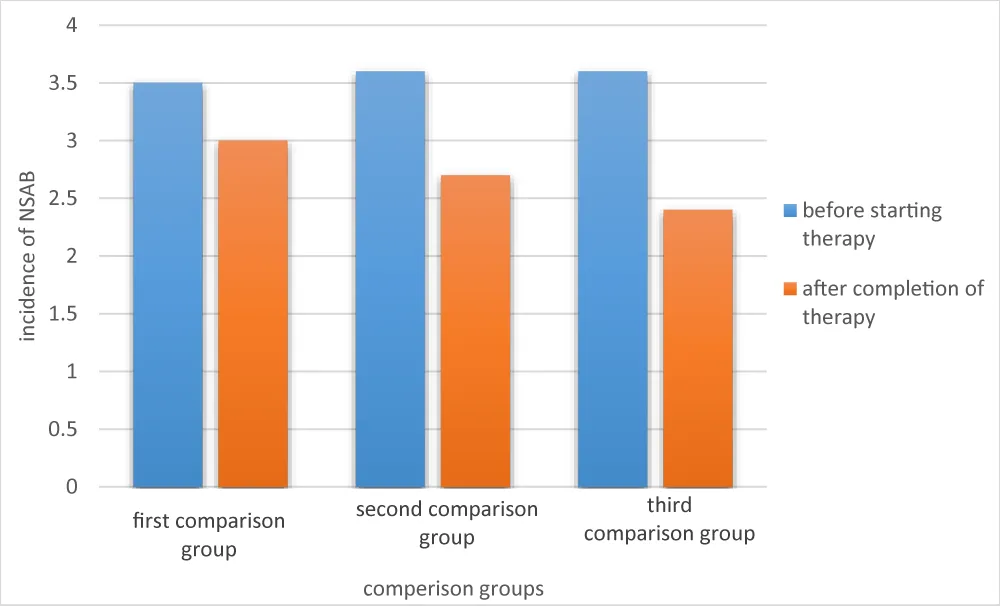
Figure 1: Changes in the frequency of non-suicidal self-harm during therapy.
The interpretation of clinical results was carried out taking into account the pharmacodynamic properties of the drugs used. The data obtained confirmed the relevance of the theory of the representative of the Russian School of Psychiatry, Professor A.V. Snezhnevsky, on general pathological rules of sidromokinesis in the form of enlargement of monoqualitative syndromes, and overlapping of process changes with exogenous-organic syndromes. At the same time, dysphoria, impulsivity, episodes of affectively narrowed consciousness still remain signs of residual-organic psychopathological changes. At the same time, the study demonstrates an increase in the proportion of catatonia as a transnosological phenomenon, including exogenous genesis [17,18]. Within the framework of the stated approach, the effectiveness of quetiapine in the treatment of urgent psychopathological conditions has been confirmed. The latter traditionally include psychomotor agitation, clinical manifestations of dysphoria, catatonia, and autoaggressive manifestations. The basis for the implementation of such a clinical effect of quetiapine is traditionally considered to be a decrease in the level of dopamine in the mesolimbic-mesocortical tract [19,20]. A positive clinical response to the use of NSAIDs in the form of diclofenac confirms the important role of post-COVID immune-inflammatory changes. The latter are realized through the activation of prostaglandin synthesis in the central and peripheral nervous system, which is a therapeutic target for NSAIDs. In this case, statistically significant increase in the clinical effectiveness of the therapy occurs only after the addition of osmotic diuretics to the basic therapy with neuroleptics and NSAIDs. Considering the ability of osmotic diuretics to realize the maximum clinical response in with regard to cerebrospinal fluid dynamics disorders and intracranial hypertension, the latter should be considered as the dominant link in the pathogenesis of psychopathological disorders in the post-COVID period in this group of patients [21-23].
Thus, the use of osmotic diuretics increases the effectiveness of therapy in the late period of coronavirus infection in patients with paranoid schizophrenia with NSAB. The issues of the relationship between endogenous and exogenous changes in the later stages of the post-COVID period remained beyond the scope of this study. It is also necessary to clarify the relationship between immune disorders, both congenital and acquired, within the framework of the scientific concept of the immune-inflammatory etiology of the development of the schizophrenic process of acquired immunity from the position of [24]. Also, the issues of comorbidity of the endogenous process and residual organic changes in the central nervous system, reflecting post-COVID and age-related changes, remain open. Finally, the prospects for more active use of nootropic and vasostabilizing drugs in this group of patients should be assessed. This, in turn, requires continued research work in such patients, using a larger statistical sample.
- Al-Kuraishy HM, Al-Gareeb AI, Al-Maiahy TJ, Alexiou A, Mukerjee N, Batiha GE. Prostaglandins and non-steroidal anti-inflammatory drugs in COVID-19. Biotechnol Genet Eng Rev. 2024;40(4):3305-3325. Epub 2022. Available from: https://doi.org/10.1080/02648725.2022.2122290
- Barlattani T, Celenza G, Cavatassi A, Minutillo F, Socci V, Pinci C, et al. Neuropsychiatric manifestations of COVID-19 disease and post COVID syndrome: the role of N acetyl-cysteine and acetyl-L-carnitine. Curr Neuropharmacol. 2024. Epub ahead of print. Available from: https://doi.org/10.2174/011570159x343115241030094848
- Nlandu Y, Tannor EK, Bafemika T, Makulo JR. Kidney damage associated with COVID-19: from the acute to the chronic phase. Ren Fail. 2024;46(1):2316885. Epub 2024. Available from: https://doi.org/10.1080/0886022x.2024.2316885
- Tassone D, Thompson A, Connell W, Lee T, Ungaro R, An P, et al. Immunosuppression as a risk factor for COVID-19: a meta-analysis. Intern Med J. 2021;51(2):199-205. Available from: https://doi.org/10.1111/imj.15142
- Peluso MJ, Deeks SG. Mechanisms of long COVID and the path toward therapeutics. Cell. 2024. Available from: https://doi.org/10.1016/j.cell.2024.07.054
- Huntington SF, Lin D, Lafeuille MH, Thompson-Leduc P, Shah A, Kim N, et al. Identification of cytokine release syndrome and indicators of severity in retrospective databases among patients receiving immunotherapy. Pharmacol Res Perspect. 2024;12(6):e70024. Available from: https://doi.org/10.1002/prp2.70024
- Raza ML, Imam MH, Zehra W, Jamil S. Neuro-inflammatory pathways in COVID-19-induced central nervous system injury: implications for prevention and treatment strategies. Exp Neurol. 2024;382:114984. Epub 2024. Available from: https://doi.org/10.1016/j.expneurol.2024.114984
- Maury A, Lyoubi A, Peiffer-Smadja N, de Broucker T, Meppiel E. Neurological manifestations associated with SARS-CoV-2 and other coronaviruses: a narrative review for clinicians. Rev Neurol (Paris). 2021;177:51-64. Available from: https://doi.org/10.1016/j.neurol.2020.10.001
- Tian T, Wu J, Chen T, Li J, Yan S, Zhou Y, et al. Long-term follow-up of dynamic brain changes in patients recovered from COVID-19 without neurological manifestations. JCI Insight. 2022;7(4):e155827. Available from: https://doi.org/10.1172/jci.insight.155827
- Li C, Verduzco-Gutierrez M. Neurologic and neuromuscular sequelae of COVID-19. Phys Med Rehabil Clin N Am. 2023;34(3):539-549. Epub 2023 Apr 6. Available from: https://doi.org/10.1016/j.pmr.2023.04.002
- Bohmwald K, Diethelm-Varela B, Rodríguez-Guilarte L, Rivera T, Riedel CA, González PA, et al. Pathophysiological, immunological, and inflammatory features of long COVID. Front Immunol. 2024;15:1341600. Available from: https://doi.org/10.3389/fimmu.2024.1341600
- Can B, Oz S, Sahinturk V, Musmul A, Alatas İO. Effects of conivaptan versus mannitol on post-ischemic brain injury and edema. Eurasian J Med. 2019;51(1):42-48. Available from: https://doi.org/10.5152/eurasianjmed.2019.18368
- Cook AM, Morgan Jones G, Hawryluk GWJ, Mailloux P, McLaughlin D, Papangelou A, et al. Guidelines for the acute treatment of cerebral edema in neurocritical care patients. Neurocrit Care. 2020;32(3):647-666. Available from: https://doi.org/10.1007/s12028-020-00959-7
- Dabrowski W, Siwicka-Gieroba D, Robba C, Bielacz M, Sołek-Pastuszka J, Kotfis K, et al. Potentially detrimental effects of hyperosmolality in patients treated for traumatic brain injury. J Clin Med. 2021;10(18):4141. Available from: https://doi.org/10.3390/jcm10184141
- Methodological recommendations “Prevention, diagnosis and treatment of the new coronavirus infection COVID-19”, version 7, 03 Jun 2020.
- Solodov AA, Petrikov SS. Effect of hyperosmolar solutions on intracranial and cerebral perfusion pressure in patients with non-traumatic intracranial hemorrhages. Rus Neurosurgical Journal named after prof. A.L. Polenov. 2009;4(4):59-65.
- Beach SR, Luccarelli J, Praschan N, Fusunyan M, Fricchione GL. Molecular and immunological origins of catatonia. Schizophr Res. 2024;263:169-177. Epub 2023 Mar 23. Available from: https://doi.org/10.1016/j.schres.2023.03.013
- Dawood AS, Dawood A, Dawood S. Catatonia after COVID-19 infection: scoping review. BJPsych Bull. 2023;47(4):208-219. Available from: https://doi.org/10.1192/bjb.2022.30
- Redon M, Virolle J, Montastruc F, Taïb S, Revet A, Da Costa J, et al. The use of antipsychotics in the treatment of catatonia: a systematic review. Eur Psychiatry. 2025;68(1):e48. Available from: https://doi.org/10.1192/j.eurpsy.2025.9
- Swain CA, Robbs EJ, Verma L, Brandt H, Seppaenen AL, Cavnar PJ. Characterization of the atypical antipsychotic drug aripiprazole cytotoxicity in the neutrophil model cell line HL-60. PLoS One. 2025;20(2):e0318878. Available from: https://doi.org/10.1371/journal.pone.0318878
- Acioglu C, Elkabes S. Innate immune sensors and regulators at the blood brain barrier: focus on toll-like receptors and inflammasomes as mediators of neuro-immune crosstalk and inflammation. J Neuroinflammation. 2025;22(1):39. Available from: https://doi.org/10.1186/s12974-025-03360-3
- Fekete M, Lehoczki A, Szappanos Á, Toth A, Mahdi M, Sótonyi P, et al. Cerebromicrovascular mechanisms contributing to long COVID: implications for neurocognitive health. Geroscience. 2025;47(1):745-779. Epub 2025 Jan 7. Available from: https://doi.org/10.1007/s11357-024-01487-4
- Talkington GM, Kolluru P, Gressett TE, Ismael S, Meenakshi U, Acquarone M, et al. Neurological sequelae of long COVID: a comprehensive review of diagnostic imaging, underlying mechanisms, and potential therapeutics. Front Neurol. 2025;15:1465787. Available from: https://doi.org/10.3389/fneur.2024.1465787
- Klyushnik TP, Zozulya SA. Immunology of schizophrenia: a modern view on inflammatory hypotheses of the disease. Psychiatry (Moscow). 2024;22(4):14-25. Available from: https://doi.org/10.30629/2618-6667-2024-22-4-14-25