
More Information
Submitted: February 09, 2026 | Accepted: February 23, 2026 | Published: February 24, 2026
Citation: Upadhyay N. Managing Hyperkinetic Disorder through Behaviour Therapy and Parent Management Training: A Case Work Approach. Arch Psychiatr Ment Health. 2026; 10(1): 014-024. Available from:
https://dx.doi.org/10.29328/journal.apmh.1001062
DOI: 10.29328/journal.apmh.1001062
Copyright license: © 2026 Upadhyay N. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Hyperkinetic disorder; ADHD; Child mental health; Behavior therapy; Parent management training

Managing Hyperkinetic Disorder through Behaviour Therapy and Parent Management Training: A Case Work Approach
Nisha Upadhyay*
Assistant Professor of Clinical Psychology, Jaipur, India
*Corresponding author: Nisha Upadhyay, Assistant Professor of Clinical Psychology, Jaipur, India, Email: [email protected]
Background: Hyperkinetic Disorder (ICD-10: F90.0) is marked by persistent patterns of inattention, hyperactivity, and impulsivity that interfere with a child’s academic, social, and adaptive functioning. Early identification and structured behavioural interventions, particularly those involving parents, play a crucial role in improving outcomes. Children with co-existing borderline intellectual functioning often present additional challenges in assessment and management.
Aim: To examine the effectiveness of Behaviour Therapy and Parent Management Training in managing symptoms of Hyperkinetic Disorder in a child with borderline intellectual functioning through a structured case work approach.
Methodology: The case involved an 8-year-old girl referred for psychological assessment due to persistent inattentiveness, restlessness, excessive talkativeness, and task incompletion. A comprehensive assessment battery was administered, including the Developmental Screening Test (DST), Vineland Social Maturity Scale (VSMS), Child Behavior Checklist (CBCL), ADHD Rating Scale, Indian Scale for Assessment of Autism (ISAA), and Malin’s Intelligence Scale for Indian Children (MISIC). Based on case history, behavioral observations, and test findings, a diagnosis of Hyperkinetic Disorder was formulated. Intervention was delivered across nine sessions, incorporating Psychoeducation, Behaviour Therapy, and Parent Management Training. Techniques such as task chunking, visual schedules, token economy, structured routines, listening games, and positive reinforcement were implemented with active parental involvement.
Results: Post-intervention, there was approximately 60% improvement in attention span and 55% reduction in hyperactive behaviors, as reported by both parents and teachers. The child demonstrated better task completion, improved listening skills, and enhanced classroom engagement. Despite borderline intellectual functioning (FSIQ = 75), structured behavioural strategies and consistent parental implementation led to significant functional improvement.
Hyperkinetic Disorder (ICD-10: F90.0) is a neurodevelopmental condition characterized by pervasive and persistent patterns of inattention, hyperactivity, and impulsivity that significantly impair academic, social, and adaptive functioning. According to the World Health Organization classification system (ICD-10), Hyperkinetic Disorder requires the presence of symptoms across multiple settings with onset before the age of seven years and clear evidence of functional impairment.
Children with hyperkinetic symptoms frequently demonstrate academic underachievement, peer relationship difficulties, emotional dysregulation, and behavioral disturbances. When associated with borderline intellectual functioning, the clinical presentation may become more complex, often complicating assessment, differential diagnosis, and intervention planning.
Behavior Therapy (BT) and Parent Management Training (PMT) are evidence-based psychosocial interventions recommended for children with ADHD/Hyperkinetic Disorder. Behavioral interventions aim to modify environmental contingencies, reinforce adaptive behaviors, and reduce disruptive behaviors through structured routines and consistent reinforcement systems. Parent Management Training equips caregivers with skills to implement structured behavioral strategies at home, thereby ensuring ecological validity and generalization of therapeutic gains.
Although pharmacological management remains common, behavioral and parent-focused interventions play a critical role, particularly in young children and in cases where medication adherence is inconsistent. However, literature from Indian clinical settings documenting structured case-based behavioral intervention approaches remains limited.
The present case study aims to examine the effectiveness of Behavior Therapy and Parent Management Training in managing Hyperkinetic Disorder in a child with borderline intellectual functioning using a structured case work approach.
Study design
This study follows a single-case clinical case work design involving detailed assessment, structured behavioral intervention, and outcome evaluation over nine therapeutic sessions.
Participant
The participant was an 8-year-old female child referred from the Department of Psychiatry for psychological assessment and therapeutic intervention due to symptoms of inattention, hyperactivity, impulsivity, and behavioral dysregulation.
Assessment procedure
A comprehensive psychological assessment battery was administered to evaluate developmental functioning, socio-adaptive skills, behavioral problems, and intellectual functioning, and to rule out differential diagnoses. The tools included:
- Developmental Screening Test
- Vineland Social Maturity Scale
- Child Behavior Checklist
- Malin’s Intelligence Scale for Indian Children
- National Institute for the Mentally Handicapped (ISAA)
Diagnosis was formulated based on ICD-10 criteria [1-4].
Intervention procedure
The intervention was conducted across nine sessions of 45 minutes each, delivered in three phases:
- Initial phase (Sessions 1–3): Assessment, rapport building, diagnostic clarification
- Middle phase (Sessions 4–7): Psychoeducation, Behavior Therapy, and Parent Management Training
- Terminal phase (Sessions 8–9): Consolidation of skills and relapse prevention planning
Outcome was assessed based on behavioral reports from parents and teachers and functional improvements in academic and home settings.
Name –A M
Age/Sex: 8/F
Education: UKG
Occupation: Student
Father’s name: S M
Father’s occupation: Teacher
Brought to hospital by: Father and Mother
Source of referral: Department of Psychiatry
Purpose- Psychological assessment and therapeutic intervention
Previous consultation: Yes
Presenting complaints
History of Present Illness (HOPI)
Mode of onset: Insidious
Course of illness: Continuous
Progress of illness: Deteriorating
Predisposing factor(s): Delayed milestones.
Limiting or modifying factor(s): Family support.
Age at which the problem was recognized: 5 years
Evolution and sequence of symptoms (narrative account):
The index child was born out of a non-consanguineous marriage with a full-term delivery at 9 months through normal birth. During the prenatal period, the adolescent’s mother was reported to be anaemic. There were no head injuries present during birth, and an immediate birth cry was present. The weight of the adolescent at the time of birth was 2.9 kgs. During the post-natal period, the child was breastfed. All developmental milestones were delayed by 3-4 months.
During her early childhood, around the ages of 3 or 4, the child started exhibiting behaviours such as running and jumping around. Whenever her parents encouraged her to engage in an activity or play with a toy, she would begin throwing toys and would start screaming. These behaviours were initially perceived as age-appropriate. The child began attending school at the age of four; however, due to the COVID-19 pandemic, she had to stay at home. Her parents attempted to engage her in studies, but she struggled to maintain focus for extended periods.
By the age of five, the child began screaming and incessantly questioning her parents. She talked excessively and exhibited stubbornness, refusing to listen to her parents’ instructions. As the child grew older, her parents became increasingly concerned that her behaviour had not ceased. She continued to scream whenever things did not go according to her liking. These situations worsened over time. Whenever her parents instructed her to sit down and study or play with toys, she would throw objects and run around excessively. She refused to stay in one place, often engaging in disruptive behaviours such as throwing and tampering with objects. She did not listen to her parents and continuously talked, frequently asking questions about everything. The child was brought to the department of psychiatry for the chief complaints of difficulty sustaining attention, excessive talkativeness and restlessness, running and jumping around, leaving activities unfinished, screaming, and showing stubbornness. Patient was referred to the Department of Clinical Psychology for further assessment.
Persistent and pervasive mood: Euthymic
Biological functions: Normal
Impact of illness on role functioning, activities of daily life, personal care, and overall attitude: The child had a significant decline in academic performance.
Negative history
No h/o suggestive of head injury, brain fever, epileptic fits, or illness related to brain dysfunction
No h/o suggestive of truancy, stealing, cruelty, bullying, or violation of rules. No h/o suggestive of defiant and provocative behavior.
No h/o qualitative disturbances in social communication, social reciprocity, and restricted behavior and stereotyped pattern of behavior.
Treatment history
In July 2023, the patient was brought to a psychiatrist and was diagnosed with attention deficit hyperactivity disorder. They adhered to the treatment for one month, but stopped due to slight relief. In September 2023, the patient was brought to a psychiatrist and was diagnosed with autism spectrum disorder. The patient adhered to the treatment for one month, but discontinued due to no improvement in symptoms [5,6].
Past medical history
No past Medical History was reported.
Psychiatric history
In July 2023, the patient received a diagnosis of attention deficit hyperactivity disorder. In September 2023, the patient received a diagnosis of autism spectrum disorder.
Family history
Type of family: Nuclear
Status of family: Intact
Consanguinity between parents: Absent
Household composition:
| S.No. | Name | Relationship | Age/Sex | Education | Occupation |
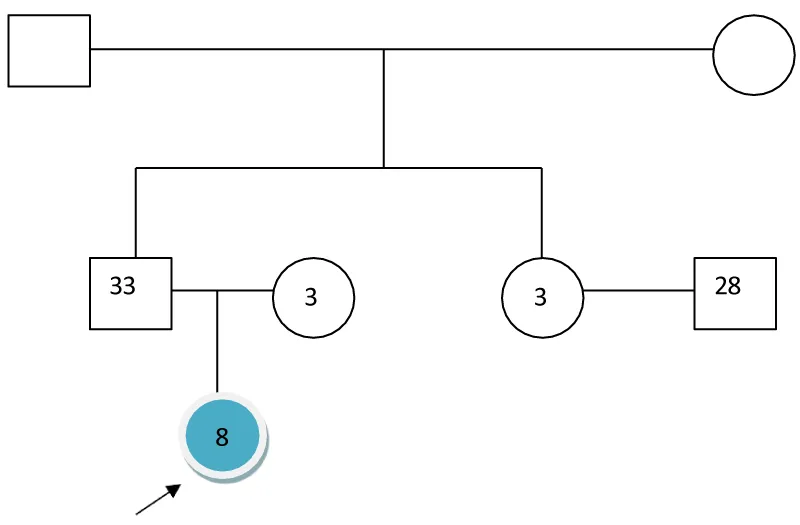
| 1. | Mr. K | Father | 33yr/M | MA | Teacher |
| 2. | Ms. N | Mother | 31yr/F | B Ed | Teacher |
The child is living in an intact, nuclear family with family members, including father and mother. She is a single child, and his relationship with family members is cordial. The family environment is congenial. No history of psychiatric illness and consanguinity was reported in the family.
Family genogram
Family history of mental and medical illness:
No history suggestive of mental and medical illness in the family.
Personal history
Prenatal History:
Planned/Unplanned Conception: Planned
Wanted/Unwanted Child: Wanted
Attempted but failed abortion/Threatened abortion/Bleeding during late pregnancy/RH Incompatibility/Trauma: No
History of gestational diabetes/Hypertension/Jaundice/Others: No
X-Ray exposure/Potentially harmful medications/Substance use/Infection/Fever/STD/: No
Nutritional status of mother during pregnancy: Normal
Fetal movements: Normal
Natal and neonatal history: Term: Full term
Delivery place: Hospital
Delivery type: Normal
Head injury during birth: No presentation: Normal prolapsed cord: No
Birth weight: Normal (2.9kg)
Birth cry: Immediate color of baby: Pink Multiple Pregnancies: No Congenital anomaly: No
Postnatal history: Infections: No jaundice: No
Feeding problems: No injury: No Convulsions: No
Feeding history: The child was breast fed till 8 months of age, no complications reported.
Developmental history:
| Gross Motor | Expected | Achieved | Fine Motor/Cognitive | Expected | Achieved |
| Neck holding | 3 months | Delayed by 4 months | Mature pincer grasp | 1 year | Delayed by 4 months |
| Stands alone | 9 months | Delayed by 4 months | Scribbles | 1 ½ years | Delayed by 4 months |
| Walks alone | 15 months | Delayed by 4 months | Copies a circle | 3 years | Delayed by 4 months |
| Runs/walks Up and down | 2 years | Delayed by 4 months | Identifies body parts | 4 years | Delayed by 4 months |
| Rides a tricycle | 3 years | Delayed by 4 months | Tells address/know Rules of zames | 5 years | Delayed by 4 months |
| Language | Expected | Achieved | Social | Expected | Achieved |
| Babbling | 6 months | Delayed by 4 months | Social smile | 2 months | Delayed by 4 months |
| Disyllables | 9 months | Delayed by 4 months | Recognizes mother | 3 months | Delayed by 4 months |
| 2–3-word sentences | 2 years | Delayed by 4 months | Stranger anxiety | 6 months | Delayed by 4 months |
| Known full name and gender | 3 years | Delayed by 4 months | Separation anxiety | 1 year | Delayed by 4 months |
| Tells a story/poem | 4 years | Delayed by 4 months | Pretend/parallel play | 2 -2 ½ years | Delayed by 4 months |
| Asks meaning of words | 5 years | Delayed by 4 months | Associative/cooperative play | 3-4 years | Delayed by 4 months |
| Self-Help | |||||
| Feeds Independently | 18 months | Delayed by 4 months | Bladder control | <5 years | Delayed by 4 months |
| Brushes teeth | 3 years | Delayed by 4 months | Dresses self | 5 years | Delayed by 4 months |
| Bowel control | <4years | Delayed by 4 months | Others, specify | ||
Immunization history: The Index child was timely vaccinated.
Home environment: The overall home environment is congenial.
Pattern of parental functioning permissiveness/rigidity: Permissive
Consistency/Inconsistency: Consistency
Strictness of discipline/liberal: Moderate discipline
Approval of interests/disapproval: Approval of Interests
Protectiveness/Non-protectiveness: Protectiveness
Tolerance of deviance/non-tolerance: Tolerance of deviance
Expectations from child: The parents are eager for their child to improve and focus on her studies.
Pattern of family dynamics: The child’s relationship is cordial with family members. Most important decisions in the family are taken by the father. The child’s family is supportive towards her and communicates in an open, direct, and clear interaction pattern. The family environment is congenial.
Reasons for the condition of the child as perceived by the family: The child’s family understands her condition and illness and shows efforts to gain knowledge to help her. Parents are worried about her condition.
Scholastic history
Type of school: Private school
Age of entry: 4 years
Schooling details: The child started going to a private school at the age of 4 years, but due to Covid 19, she had to stay at home. She is currently studying in the UKG.
Scholastic performance: (Average) As reported by the informant, the child scored average marks.
Disciplinary actions: No
Attendance: Regular
Adjustment to school: Difficulty adjusting
Peer group adjustment: Poor, as she has difficulty following the rules of the games and has difficulty initiating and maintaining conversations
Relations with authority: Inadequate, as her teacher reports that she struggles to stay in one place and she’s not able to focus on her studies.
Parental satisfaction with child’s performance: Inadequate
Reading/writing/arithmetic skills: Adequate
Habits, interests, and talents of a child: The child likes to play with dolls and watch cartoons.
Playhistory
Play behavior: Enjoys play
Reasons for poor play behavior: Less social interaction and difficulty following rules
Play preferences: Plays alone or plays with cousin, younger sister, and peers if they are around.
Knowledge of games governed by rules: poor Behavior while playing in-group situations: Poor. Leisure time activities: Plays with dolls
Sexual and marital history: NA
Occupation history: NA
Forensic history: NA
Temperament
Source of information and its reliability: Mother and Father, reliable
Activity level: The index adolescent’s activity level is moderate, and she moves around, runs, and walks.
Attention span and persistence: She is usually persistent, and her attention span is poor.
Approach withdrawal: She seems to like it when exposed to new events that are of her interest.
Adaptability: The child takes time to adapt to new situations and responds well to changed circumstances.
Distractibility: She is easily distracted but can sustain attention when she is engrossed in a task she is interested in.
Intensity of reaction: The child has a high reaction to objects and things of interest to her.
Threshold of responsiveness: The child is not bothered by pain, noise, or other sensations.
Quality of mood: The quality of the child’s mood is usually happy.
Rhythmicity: The child’s rhythmicity was fixed, but she could sustain if there were slight changes in the routine.
Impression – Difficult Temperament
Behavioural observation
General appearance
General physical appearance: Kempt and tidy
Estimate of age: Appropriate
Body built: Ectomorph
Touch with surrounding: Present
Eye contact with the examiner: Partially maintained
Dress: Appropriate
Facial expression: Smiling
Posture: Sitting on the edge of chair; constantly moving
Relationship capacity and sociability
The child does not get distressed when separated from parents. She was hesitant during the initial phase of the interview, but became comfortable and cooperative as the interview proceeded. She maintained eye contact partially and was cooperative in the interview; rapport was established easily.
Spontaneous motility and activity level: hyperkinetic
Motor behavior: Restless
Speech
Intensity: Audible Pitch: Normal Quality: Normal Prosody: Maintained
Reaction time: Normal Speed: Normal
Ease of speech: Was speaking constantly. Speech was relevant
Speech was coherent
Speech was not goal-directed. Productivity: decreased. Normal Deviation not found.
Mood and affect
Objective: Euthymic Intensity of affect: Normal Mobility of affect: Normal Range of affect: Full range Reactivity: Normal Communicability: Normal Appropriate
Diurnal variation of affect: Not present
Attention span and distractibility: Attention was aroused but not sustained
Intellectual capacity: Borderline level of intellectual functioning
Stated interests and content of thought: No abnormality was found.
Play behavior: The child prefers physically active games like running and jumping. She finds it difficult to wait for her turn when playing with other children. She starts playing a game or toy enthusiastically, but quickly loses interest, jumping to a different activity before finishing the previous one.
Test behaviour
The index child was kempt and tidy, and looked appropriate to her age. Her attention was aroused but not sustained. Rapport was established easily. She was oriented to person, place, and time. High motor activity was present. The child was constantly moving around during the interview. She had trouble concentrating. The child was able to follow instructions on the tasks, which were according to her preference.
Tools administered & rationale
The formal assessments were carried out to better understand the child’s current condition and clarify the diagnosis. The tools administered consist of –
- Development Screening Test (DST): The rationale for using DST is to assess the child’s developmental functioning, as the case history is suggestive of delays in developmental milestones.
- Vineland Social Maturity Scale (VSMS): The rationale for using VSMS is to understand the child’s social and adaptive capacities, as this case history is suggestive of difficulties in carrying out tasks independently, problems in verbal communication, and initiating social relationships.
- Child Behaviour Checklist (CBCL): To assess the presence of behavioural and emotional problems.
- ADHD rating scale: To assess the presence and symptoms of ADHD
- Indian scale for assessment of autism: To assess the presence and severity of autistic symptoms as the patient was diagnosed with autism.
- Malin’s Intelligence Scale for Indian Children (MISIC): It is the intelligence test, which includes both verbal and non-verbal tests, used for Indian children. The rationale for using this test was to assess the intellectual functioning as case history indicative of poor academic performance, lack of concentration, and to be sure if the difficulties are due to low intellectual capacity or behavioral issues. It was also administered to identify strength areas for better academic performance [7].
Test findings
- Developmental Screening Test (DST): Upon administration of the Developmental Screening Test, the child’s developmental age was found to be 7 years 9 month and her Developmental Quotient (D.Q) was 96.8, which is indicative of an average level of developmental functioning [8].
- Vineland Social Maturity Scale (VSMS): Upon administration of the Vineland Social Maturity Scale, the child’s social age was found to be 7 years 12 months and Social Quotient (S.Q) of 108.12, which is indicative of an average level of socio-adaptive functioning. The profile analysis is followed as [9]:
- Child Behavior Checklist (CBCL): Upon administration of child behavior checklist, the child obtained a T score of 45 in internalizing, t score of 64 in externalizing, and a T score of 23 in other problems. The child obtained a score of 8 in social problems, like the patient's difficulty getting along with others, she is clumsy in handling things, 13 in attention problems, like fails to finish tasks, can't concentrate for a long time and 13 in aggressive behavior as she argues and screams a lot, which is indicative of presence of symptoms in clinical range.
- ADHD rating scale: Upon administration of the ADHD rating scale, the child scored 7 in inattention, which is indicative of the presence of inattention, and a score of 9 in impulsivity and hyperactivity, which is indicative of the presence of hyperactivity.
- Indian Scale for Assessment of Autism (ISAA): On the Indian Scale for Assessment of Autism child’s scores are as follows-
- Malin’s Intelligence Scale for Indian Children (MISIC): On administration of Malin’s intelligence scale for Indian children, the child obtained a TQ on the verbal scale was 78.8 and on the performance task, the child obtained a T.Q. of 71.2. The full-scale IQ of 75 is indicative of borderline intellectual functioning. However, the child was showing distractibility and hyperactive behavior, which could have affected the child’s performance.
| DOMAINS | AGE ATTAINED (YEARS) | SOCIAL QUOTIENT |
| Self-help general | 96 months | 100 |
| Self-help eating | 120 months | 125 |
| Self-help dressing | 120 months | 125 |
| Self-direction | 64 months | 66.6 |
| Occupation | 108 months | 112.5 |
| Communication | 96 months | 100 |
| Locomotion | 120 months | 125 |
| Socialization | 72 months | 75 |
| Domains | Scores |
| Social Relationship & Reciprocity | 10 |
| Emotional Responsiveness | 5 |
| Speech, Language & Communication | 9 |
| Behavioural Patterns | 9 |
| Sensory Aspects | 6 |
| Cognitive Component | 4 |
The total score was 43.
Impression: Test findings indicate that the child does not have autism.
| Verbal table | Raw score | T.Q. | Performance Test | Raw score | T.Q. |
| Information Test | 6 | 75 | Picture completion | 4 | 70 |
| General Comprehension Test | 4 | 75 | Block design | 2 | 57 |
| Arithmetic Test | 4 | 75 | Object assembly | 4 | 65 |
| Similarity Test | 6 | 95 | Coding (A) | 11 | 70 |
| Vocabulary Test | 12 | 74 | Mazes | 10 | 94 |
| Sum of verbal test | 394 | Sum of performance Test | 356 |
| Scale | T.Q. |
| Verbal scale | 78.8 |
| Performance scale | 71.2 |
| Full scale | 75 |
Strength areas - The child scored high T.Q. score in Similarity Test and Mazes, indicative of high ability to form verbal concept formation, reasoning, and planning skills.
Areas of limitations - The child scored a low T.Q. score in Picture completion, Block design, Object assembly, and Coding (A), indicative of poor ability to differentiate between essential and non-essential information and concept formation.
Summary of test findings
The child obtained a score of was 96.8 on developmental screening test, which is indicative of average level of deficit in developmental functioning, 108.12 on Vineland social maturity scale which is indicative of average level of socio-adaptive functioning, on Child behavior checklist, a score of 8 in social problems, 13 in attention problems and 13 in aggressive behavior which is indicative of presence of symptoms in clinical range, on ADHD, 7 in inattention and 9 in impulsivity and hyperactivity which is indicative of presence of ADHD symptoms, 57 in Indian scale for assessment for autism, which indicates absence of autism in the child, full scale IQ of 75 on Malin’s intelligence scale for children indicative of borderline intellectual functioning.
Test impression
Based on the case history, behavioral observation, and psychological test findings indicate that the child is having a borderline level of intellectual functioning with ADHD symptoms.
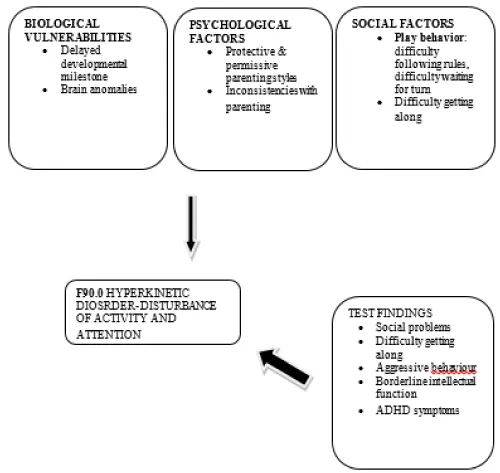
Diagnostic formulation
The index child is an eight-year-old Hindu studying in U.KG from a middle SES family of Jaipur, Rajasthan, with a family history suggestive of the mother being anemic during the prenatal period, personal history suggestive of difficult temperament and developmental delays of 4 months in every domain, play history suggestive of engaging in games with peers and siblings but does not know games governed by rules and behavior is poor in in-group situations, school history suggestive of difficulty following instructions and classroom rules, parents satisfaction with child performance is inadequate, has come now accompanied by her mother and father, history being reliable and adequate with illness of four years duration, preceded by delayed milestones with insidious onset, continuous course, and deteriorating progress of illness, characterized by difficulty sustaining attention, excessive talkativeness, excessive restlessness, running and jumping around, leaving activities unfinished, screaming and stubbornness.
Behavioral observation findings reveal partially maintained eye contact, hyperactive and restless motor behavior, non-gold directed speech with decreased productivity, borderline level of intellectual functioning.
DiagnosisProvisional diagnosis: F90.0: Hyperkinetic Disorder – Disturbance of activity and attention
Points in favor
- Impaired attention and over activity
- Early onset of behavior problems
Case conceptualization
Management plan
- Psychoeducation
- Behavior Therapy (BT)
- Parent management training (PMT)
Objectives
Short-term goals:
- Enhance the parents' understanding of ADHD
- Increase Attention Span
- Improve Listening Skills
- Dealing with hyperactivity
Long-term goals:
- Sustain Attention during Schoolwork
- Support Parental Strategies for Consistency
Approaches and techniques with rational
Psychoeducation: Psychoeducation aims to help the parents understand ADHD, its impact, and strategies for management. Given the child’s history of attention difficulties, impulsive behaviors, and restlessness, psychoeducation has focused on the following: Understanding ADHD, Normalizing the Experience, Empowering the Parents and Child, Setting Realistic Expectations, etc.
Behavior therapy: Behavior therapy is essential for managing the core symptoms of ADHD, including impulsivity, inattentiveness, and hyperactivity. It focuses on modifying the environment and behaviors through structured routines, positive reinforcement, and consistent consequences. Given the child’s history of disruptive behavior, including running, jumping, throwing objects, etc., behavior therapy was used to Reinforce Positive Behaviors, Decrease Disruptive Behaviors, and involve parents in implementing strategies at home, such as using consistent rules, routines, and rewards.
Parent Management Training (PMT): Parent Management Training (PMT) teaches parents specific behavioral strategies to manage their child’s ADHD-related behaviors. Techniques include setting clear expectations, consistent use of rewards and consequences, positive reinforcement for desired behaviors, and structured routines. Parents are guided on how to give effective instructions, use time-outs for disruptive behaviors, and implement token systems to reinforce attention and task completion.
Intervention process
Initial phase: The initial phase consisted of sessions 1-3. The session was conducted offline, in the Department of Clinical Psychology, Mahatma Gandhi Hospital, with a duration of 45 min each. The session comprised the therapist, patient, and informants. The child has come to the hospital accompanied by her father and mother with the chief complaints of difficulty sustaining attention, excessive talkativeness and restlessness, running and jumping around, leaving activities unfinished, screaming, and showing stubbornness. The goal of sessions 1-3 was to clarify symptoms, conducting assessment for diagnostic clarification, and make a definite diagnosis. For clarification of symptoms, a detailed case history and temperament history were explored with the informants and also through behavioural observation of the child. Further, the session focused on establishing rapport and a good therapeutic alliance. In the second session, an assessment was conducted for clarification of symptoms and diagnosis. Child developmental and socio-occupational functioning was assessed, which was followed by an IQ assessment. Later, patient symptom severity was assessed.
Middle phase: The middle phase included sessions 4-7 and was conducted offline in the Department of Clinical Psychology. The sessions comprised the therapist, patient, and parents. At the beginning of the session, the focus was on rapport building, understanding, and reducing the distress patient’s parents regarding her symptoms, and building a good therapeutic alliance. In the psycho- education session, focus was on educating the parents about Attention-Deficit/Hyperactivity Disorder (ADHD) and providing a deeper understanding of how it affects their child’s behavior, emotional well-being, and overall development. We began by discussing how ADHD manifests through core symptoms of inattention, hyperactivity, and impulsivity. Inattention can make it difficult for the child to focus, follow through on tasks, and stay organized, often leading to challenges in school and daily responsibilities. Hyperactivity might present as constant movement, fidgeting, or an inability to stay seated, which can be disruptive in both the classroom and the home environments. Impulsivity, such as acting without thinking or difficulty waiting for turns, may lead to problems with peer relationships, frustration, and social isolation. We explored how these behaviors, while unintentional, can interfere with academic performance, resulting in missed assignments, incomplete tasks, and underachievement despite the child’s potential.
After psychoeducation, we began by discussing how to help the child focus on tasks, particularly in school and during homework. The therapist explained the importance of breaking tasks into smaller, manageable steps. For example, instead of telling her to “finish all your homework,” parents were advised to break it into specific tasks, such as “complete five math problems,” and take short breaks in between. We also explored using visual aids like a timer or a checklist to keep her engaged and aware of progress. The parents mentioned how she gets distracted easily while doing her assignments, so we discussed setting up a designated, quiet space with minimal distractions to support her attention span. At the end of the session, parents were given an attention enhancement worksheet.
The next session focused on improving the child’s listening skills. The therapist emphasized the importance of clear and concise communication to enhance her ability to listen and follow instructions effectively. The therapist suggested that parents use short, simple phrases when giving directions, such as “Please pick up your toys,” instead of longer sentences that might overwhelm her, like “Can you please clean up your room and put all your toys away?” This clarity helps the child understand expectations more easily. The therapist also explored the idea of implementing a “listening game.” In this activity, the parent gives a command—such as, “Touch your nose and then clap your hands”—and the child must repeat back the sequence to reinforce active listening. This not only encourages her to pay attention but also makes the process fun and engaging. Additionally, the therapist recommended creating a “listening jar,” where the child earns a token or sticker each time she successfully listens and follows a direction, which can accumulate toward a small reward, like extra playtime or a special treat.
To further improve focus, parents were encouraged to establish a distraction-free environment when giving instructions. This could include turning off the TV, putting away toys, or even using a quiet room to minimize background noise. For instance, parents might set a routine where they gather the child for important tasks, such as homework or chores, in a designated quiet area with no distractions. We also discussed the significance of using visual cues alongside verbal instructions. Parents can create a simple visual chart with pictures illustrating tasks, such as a picture of a backpack for “get ready for school” or a plate for “set the table.” This reinforces the verbal instruction and provides a visual reminder. Positive reinforcement was another critical point. The therapist recommended that parents praise the child immediately when she listens and follows directions correctly, using specific language like, “I’m so proud of you for listening and helping to clean up!” This immediate acknowledgment not only celebrates her efforts but also motivates her to continue improving her listening skills. The parents were left with practical strategies to implement at home, including structured games, visual aids, and positive reinforcement techniques, all aimed at fostering better listening behaviors in their child.
In our next session, we delved deeper into strategies for managing the child’s hyperactivity. The therapist emphasized the critical role of a structured environment at home in helping the child feel more secure and focused. The therapist suggested that parents implement a consistent daily routine, which could include set times for homework, play, and relaxation. For example, having a designated homework time from 4:00 to 5:00 PM can create a predictable structure, making it easier for the child to transition from school to home.
To further aid transitions, we explored the use of a visual schedule that outlines daily activities. Parents could create a colorful chart featuring images or icons representing each activity—like a picture of a book for homework, a ball for playtime, and a bed for bedtime—allowing the child to anticipate what comes next. This approach can reduce the likelihood of hyperactive outbursts during transitions. The therapist also emphasized the importance of positive reinforcement. The parents were encouraged to identify specific moments of calm behavior, such as sitting quietly during dinner or completing a task without interruption. They could use praise like, “I’m so proud of you for staying calm during dinner!” or reward the child with stickers on a chart that leads to a small prize or special outing after a certain number of stickers are earned. This approach helps to reinforce desired behaviors and encourages the child to replicate them. Overall, parents left the session equipped with practical tools and examples they could implement at home, empowering them to better support their child’s needs while managing hyperactivity.
Terminal phase
Sessions 8-9 were the terminating sessions, which involved the patient, therapist, and the parents. The termination phase began with reviewing the skills taught to the parents. The session remains focused on the long-term goal of sustaining attention during schoolwork. The client has made encouraging progress in her ability to remain focused on tasks, both at home and in the classroom. For example, during a recent math class, she was able to complete a worksheet independently by following a visual schedule and using the task chunking technique. Previously, she would need multiple reminders to stay on task, but now she requires fewer prompts and is demonstrating increased self-regulation during academic activities. To support her sustained attention, we reinforced the use of structured breaks after every 15-20 minutes of focused work, allowing her to reset before continuing with tasks.
In the next session therapist focused on supporting the parents in maintaining consistency with behavior management strategies at home, as this is critical for the child’s long-term progress. The parents were reminded of the open-door policy, where they are encouraged to reach out as needed for additional support. A monthly booster session was planned to check in child’s ADHD symptoms and to help the parents refresh the skills they have learned in therapy.
Following nine sessions of structured intervention, clinically meaningful improvements were observed across behavioral domains.
There was an approximate 60% improvement in sustained attention during structured academic activities as reported by both parents and teachers. The child demonstrated increased task completion, reduced distractibility, and improved compliance with instructions.
Hyperactive behaviors showed approximately 55% reduction, reflected in decreased running, jumping, excessive talking, and disruptive motor activity during home and classroom routines.
Improvement was also noted in listening skills, transition management, and adherence to structured routines. Parents reported enhanced confidence in managing behaviors using reinforcement-based strategies.
Despite borderline intellectual functioning (FSIQ = 75), structured behavioral intervention and consistent parental implementation led to functional improvement in academic engagement and social participation.
Outcome
There has been a notable reduction in the patient’s inattentiveness, particularly during schoolwork and structured tasks at home. With consistent routines and strategies, her ability to sustain attention has improved by approximately 60%, as reported by both parents and teachers. There was 55% reduction in her hyperactive symptoms. The reduction in hyperactivity has contributed significantly to her overall improvement, enabling her to better engage in academic and social environments.
Future plan
Booster sessions for both the patient and her parents have been scheduled once a month. These sessions will serve as a check-in to monitor the child’s progress, review the coping strategies learned during therapy, and address any new challenges that may arise. The focus will remain on maintaining her improvements in attention, behavior regulation, and social skills, while ensuring her parents continue to implement consistent strategies at home. Additionally, the patient and her parents were reminded of the open-door policy and encouraged to contact the therapist whenever needed for extra support or guidance outside of scheduled sessions.
Long-term sustainability and adjunct considerations
Although short-term outcomes were encouraging, long-term sustainability of treatment effects remains an important consideration. Evidence suggests that Parent Management Training programs typically require sustained reinforcement over extended periods, often ranging from 6 months to 1 year, with periodic booster sessions to maintain gains. For long-term stability (1–3 years), consistent implementation of structured routines, reinforcement strategies, and school collaboration is essential.
Monthly booster sessions have been planned to monitor symptom progression and reinforce parental strategies.
Additionally, emerging literature highlights the potential adjunctive role of nutritional interventions in children with hyperactivity. Balanced diets rich in omega-3 fatty acids, adequate protein intake, and reduction of excessive refined sugars may support cognitive functioning and behavioral regulation. While nutritional intervention was not formally implemented in the present case, parents were advised regarding maintaining balanced dietary habits to complement behavioral management strategies.
Further longitudinal follow-up would be beneficial to evaluate maintenance of gains over extended periods.
The present case study demonstrates that structured Behavior Therapy combined with Parent Management Training can produce significant functional improvements in children diagnosed with Hyperkinetic Disorder, even in the presence of borderline intellectual functioning.
Targeted behavioral strategies, structured routines, visual aids, and consistent parental reinforcement contributed to measurable reductions in inattentiveness and hyperactivity. Active parental involvement emerged as a critical factor in ensuring generalization of skills across home and school environments.
The findings underscore the importance of early identification, comprehensive assessment, and structured psychosocial intervention in managing Hyperkinetic Disorder. Continued follow-up and booster sessions are essential to sustain therapeutic gains over time.
- National Institute for the Mentally Handicapped. Indian scale for assessment of autism (ISAA) manual. Secunderabad: NIMH; 2009.
- Sadock BJ, Sadock VA, Ruiz P. Kaplan & Sadock’s synopsis of psychiatry: behavioral sciences/clinical psychiatry. 11th ed. Philadelphia: Wolters Kluwer; 2015. Available from: https://psychiatry.lwwhealthlibrary.com/book.aspx?bookid=1234
- Sethi N. Clinical psychology: case history taking and mental status examination. New Delhi: Pearson Education; 2013.
- Shah R, Sharma A, Grover S, Sachdeva D, Chakrabarti S, Avasthi A. Parent skills training for families of children with attention-deficit/hyperactivity disorder. 2nd ed. Chandigarh (IN): Department of Psychiatry, Postgraduate Institute of Medical Education and Research; 2020.
- Miltenberger RG. Behavior modification: principles and procedures. 6th ed. Boston: Cengage Learning; 2016. Available from: https://studylib.net/doc/26025196/behavior-modification---miltenberger
- Malin AJ. Malin’s intelligence scale for Indian children (MISIC). New Delhi: Indian Psychological Corporation; 1971. Available from: https://www.scribd.com/document/787501652/MALINS-INTELLIGENCE-SCALE-FOR-INDIAN-CHILDREN-2
- Bharatraj J. Developmental screening test (DST) manual. New Delhi: Psychological Corporation of India; 1992.
- Malin AJ. Vineland social maturity scale (Indian adaptation) manual. New Delhi: Indian Psychological Corporation; 1965.
- Achenbach TM, Rescorla LA. Manual for the ASEBA school-age forms & profiles. Burlington (VT): University of Vermont, Research Center for Children, Youth, & Families; 2001. Available from: https://www.scribd.com/document/839848767/Manual-for-the-ASEBA-School-Age-Forms-Profiles