Submitted: April 29, 2026 | Accepted: May 07, 2026 | Published: May 08, 2026
Citation: Surduleasa E, Ghinescu MC, Streinu GA, Bealcu F. Clinical and Etiopathogenic Perspectives in the Management of Autism in General Practice. Arch Psychiatr Ment Health. 2026; 10(1): 44-48. Available from:
https://dx.doi.org/10.29328/journal.apmh.1001066
DOI: 10.29328/journal.apmh.1001066
Copyright license: © 2026 Surduleasa E, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: ASD screening; ASD in children; Early diagnosis; General practice
1Faculty of Medicine, ‘Titu Maiorescu’ University, Bucharest, Romania
2Bucharest University of Economic Studies, Faculty of Management, Bucharest, Romania
*Corresponding author: Bucharest University of Economic Studies, Faculty of Management, Bucharest, Romania
Autism spectrum disorder (ASD) is a complex neurodevelopmental disorder, characterized by deficits in social communication, interaction, and repetitive/restrictive behaviors, with increasing prevalence (1 in 31 children in the USA, 3.4 times more common in boys). This review aims to highlight the current view on the prevention and early screening of autism in primary healthcare, along with the impact of the pathology on the individual and family. Although diagnosis and intervention often remain delayed, the role of the family doctor is essential for suspecting the diagnosis, combating stigma, identifying modifiable risk factors, and guiding referral for specialized evaluation. Early initiation of therapy, accompanied by complementary therapy (melatonin, probiotics), improves the prognosis.
Autism Spectrum Disorder (ASD) currently represents one of the most complex and heterogeneous neurodevelopmental disorders with a clear genetic influence. It is characterized by a series of neurobehavioral deficits, including impaired communication and social interaction skills, restrictive or repetitive behavioral stereotypies, with persistent symptomatology and onset in the early developmental period.
According to a recent report published by the Centers for Disease Control and Prevention (CDC) in the United States, a study conducted across multiple American states in 2022 identified an ASD prevalence of 32.2 per 1,000 children aged 4–8 years (1 in 31), with prevalence being higher in boys than in girls [1].
Technological advances in medicine, numerous endophenotypic cohort studies, and large-scale sharing of databases have contributed to in-depth research and validation of multiple genes associated with ASD, providing new insights into characteristic neurodevelopment. However, ASD exhibits wide variations in behavioral manifestations and cognitive profiles, which complicates the identification of dominant risk factors and pathogenic mechanisms [2].
This review aims to highlight and identify the main aspects of the contemporary approach to the prevention and early diagnosis of autism in primary care, as well as the impact of this pathology on the individual’s health status and that of their family.
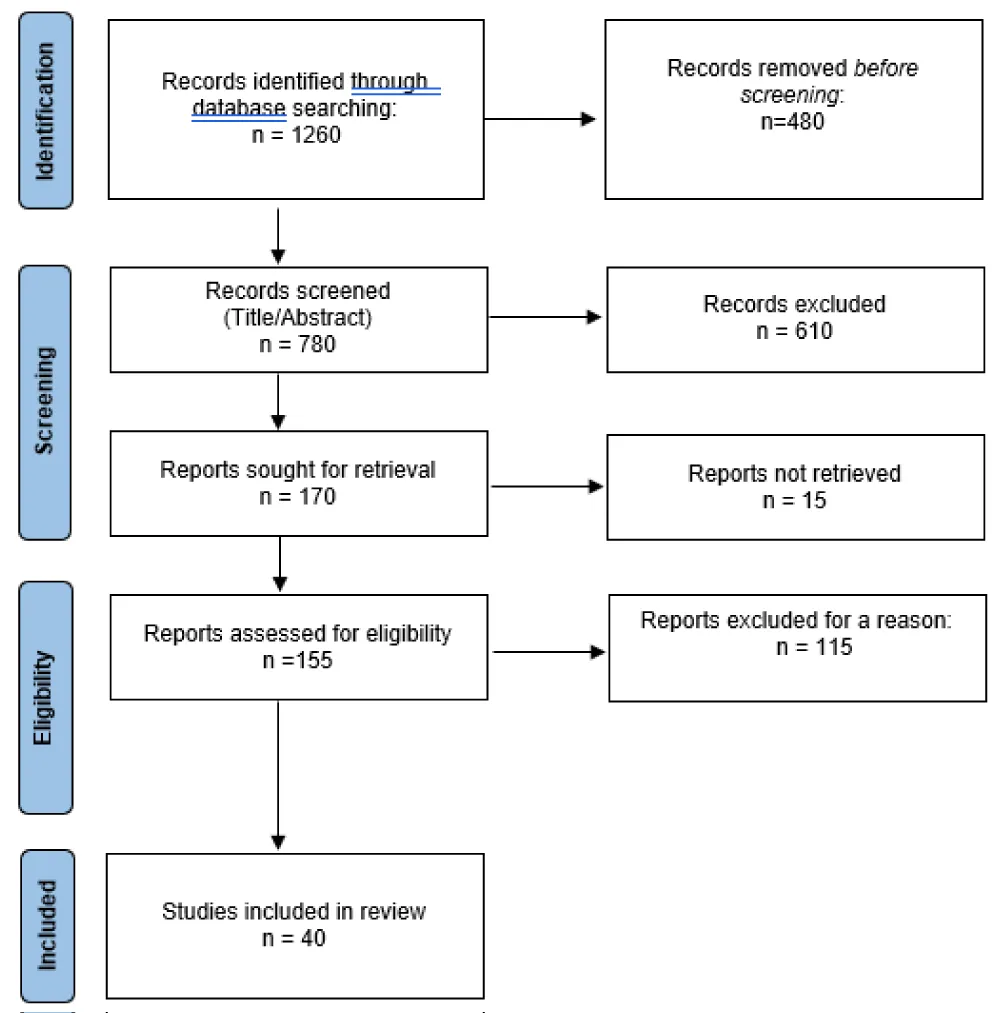
To create this review, the following platforms and search engines were used: PubMed, Elsevier, and Springer Nature. For better identification of relevant studies published between 2020 and 2026, a series of keywords was employed, such as ASD screening, ASD in children, early diagnosis, and general practice. The article selection followed the PRISMA guidelines. The information was systematized, emphasizing the main aspects of the contemporary perspective on autism in primary medical care.
The systematic search yielded an initial pool of 1260 records published between 2020 and 2026. After removing duplicates and screening titles and abstracts for relevance to primary care settings, 155 reports were sought for full-text retrieval. Following a rigorous eligibility assessment based on the inclusion of both clinical management strategies and etiopathogenic discussions, 40 studies were selected for final synthesis.
Despite recommendations for universal ASD screening at 18 and 24 months using tools such as the M-CHAT-R/F, implementation in primary care remains inconsistent, with completion rates ranging from 40–70%. Structured screening and brief training enabled primary care providers to achieve good accuracy in early identification, with diagnostic agreement rates of 75–80% compared to specialists. Fast-track triage models reduced the median age at diagnosis to approximately 33–38 months [3-5].
The general practioner’s role has evolved from a simple gatekeeper to a coordinator of complex, multi-systemic care that accounts for both behavioral symptoms and underlying biological drivers. Despite the availability of screening protocols, GPs cite limited consultation time (average 10–15 minutes) and a lack of standardized pathways for etiopathogenic testing as the primary obstacles to comprehensive autism management in primary care [6].
Collaborative research is crucial for advancing our understanding of ASD. Multidisciplinary collaborations integrate expertise from genetics, neuroscience, psychology and clinical medicine (general practice, pediatrics), enhancing research outcomes and facilitating the translation of findings into clinical practice, thus a higher quality of life for the patient and his family.
Despite the increasing prevalence, as well as greater public and professional-medical awareness, the diagnosis and selection of optimal treatment methods for ASD are often relatively delayed in the course of the disease. The social deficits associated with ASD can have negative effects on the learning process and academic achievement, as well as difficulties in coping with changes, organizational processes, or planning, potentially leading to social isolation. Consequently, in adulthood, a large number of individuals with ASD struggle to achieve independent living. Therefore, we consider it vitally important for these patients to benefit from early diagnosis and intervention.
The family physician, acting as a mediator between the medical world and the community, has the role of combating stigma and misconceptions against people with disabilities. This enables them to benefit from societal support, understanding, and involvement, thus avoiding marginalization. These measures can also increase the schooling rate of patients with ASD, as the likelihood of being bullied by peers or becoming victims of violence is higher when they attend mainstream schools rather than specialized ones [7].
Studies have shown that family physicians are reluctant and often do not implement autism screening during the 18- and 24-month visits. The reasons may include:
1. Lack of knowledge regarding the pathology, as demonstrated by a 2020 study in which only 23% of family physicians reported having adequate knowledge about these disorders [8];
2. Lack of time, since within the minutes allocated to a consultation, the physician must address general hygiene-dietary recommendations, vaccination administration, and parental concerns [6].
According to the specialized literature, the family physician has the responsibility to provide prevention and counseling to future parents, as the following non-genetic etiological risk factors have been identified:
a) Advanced parental age: There is a suggested association between advanced parental age and an increased probability of de novo mutations, more frequently of paternal origin. These effects may also be intergenerational; studies have shown that advanced grandpaternal age (on both maternal and paternal sides) is linked to ASD. From a neurobiological perspective, advanced paternal age has been associated with reduced cortical thickness in the posterior cingulate cortex, which favors decreased cognitive introspection, increased attention to the external environment, difficulty in memory retrieval and organization, and behaviors specific to ASD [9].
b) Severe maternal obesity and diabetes mellitus: These may impact fetal neurodevelopment through processes including neuroinflammation, increased oxidative stress, insulin resistance, dysregulated glucose and leptin signaling, defective serotonergic and dopaminergic signaling, disturbances in synaptic plasticity, and alterations in DNA methylation [10].
c) Infections during pregnancy: These activate the maternal immune system and, according to studies, play a role in triggering ASD through cytokine signaling that crosses the placenta, potentially causing numerous adverse neuronal effects in the developing fetal brain [10].
d) Stress, smoking, and alcohol consumption [11].
e) Deficiencies in vitamin D, iron, folate, or zinc: These may lead to neural tube defects [11].
Observation of warning signs should be performed at every medical visit by the family physician, thereby complementing the clinical examination of the infant. Among the signs that may indicate (but do not confirm) ASD pathology are: [12].
The early screening methods validated by the specialized literature that can be applied in primary care to subsequently refer the patient to a specialist for diagnostic confirmation are:
a) M-CHAT-R/F Questionnaire: Completed by the parent, consisting of 20 questions. It has demonstrated high sensitivity in identifying children aged 16–30 months who require further evaluation, detecting a significant proportion of children who would otherwise remain undiagnosed until school age [13].
b) Screening Tool for Autism in Toddlers and Young Children (STAT): An interactive screening tool designed for children aged 24–36 months. It takes approximately 20 minutes and consists of 12 activities aimed at assessing play, communication, and imitation skills [14].
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM), the formulation of a nosological diagnosis takes into account the following criteria, manifested at the time of evaluation or historically: [15].
A. Persistent deficits in social communication and social interaction across multiple contexts:
B. Restricted, repetitive patterns of behavior, interests, or activities — at least two of the following:
C. Symptoms must be present in the early developmental period.
D. Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning.
E. These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay.
In addition to psychiatric and neurological comorbidities, a significant proportion of somatic disorders have been documented in patients with ASD, such as gastrointestinal manifestations (four times more frequent than in the general population: gastroesophageal reflux, constipation), food allergies, and autoimmune conditions (e.g., psoriasis) [16].
The care of patients with ASD is based on an interdisciplinary approach. To date, no treatment modality offers a curative perspective for ASD. Currently available treatments include Applied Behavior Analysis (ABA), social skills training, occupational therapy, physical therapy, sensory integration therapy, and assistive technology. Early and intensive behavioral intervention is recommended for at least 25 hours per week in preschool-aged children [17].
According to studies, complementary therapies that may be used or recommended in family medicine practice include:
The transition from childhood/adolescence to adulthood in individuals with autism is a critical period both medically and socially, as they may face challenges in areas such as employment and socio-economic independence. Family physicians play a central role in facilitating this transition by collaborating with patients and their families to develop comprehensive plans and connect them with appropriate services.
The first contact of families with a child healthcare specialist is usually the family physician/pediatrician. Three of the most common parental concerns expressed are: speech delay, deficits in understanding instructions/directions, and hyperactivity. These observations are not exclusive to ASD, but should be considered by the attending physician, with appropriate referral of the family for specialist evaluation.
Children with ASD must benefit from a multidisciplinary diagnostic and therapeutic approach for the early identification and appropriate treatment of all medical problems.
The family-centered care approach emphasizes that autism affects not only the individual but the entire family unit. Family physicians are encouraged to provide support and resources to parents and siblings and to assist families in navigating complex health and education systems.
Despite the systematic approach, this review acknowledges several limitations inherent in the current body of literature. There is a lack of standardized longitudinal data linking early interventions led in general practice directly to long-term etiopathogenic outcomes, making it difficult to quantify the precise biological impact of primary care management. Additionally, much of the recent literature is centered on high-income healthcare systems; thus, the generalizability of these clinical pathways to low-resource settings remains limited.